Child's Medical History
Begin by asking the caregiver about symptoms and key background information:
- Ear pain or discomfort
- Hearing loss or delayed response to sounds
- Balance issues or dizziness
- Speech or language delays
- Breathing difficulty, snoring, or nasal congestion
- Swallowing difficulties
- Past ENT problems or recurrent infections
- Recent trauma to the ear, nose or throat
Physical Examination
Ears
Use an otoscope to assess the ear canal and tympanic membrane. Look for:
- Redness, swelling or discharge
- Tympanic membrane perforation
- Foreign bodies
- Signs of infection or inflammation
- Hearing abnormalities (whisper test / tuning fork)
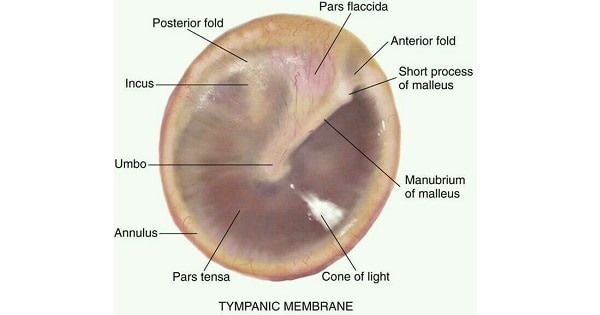
Normal Tympanic Membrane
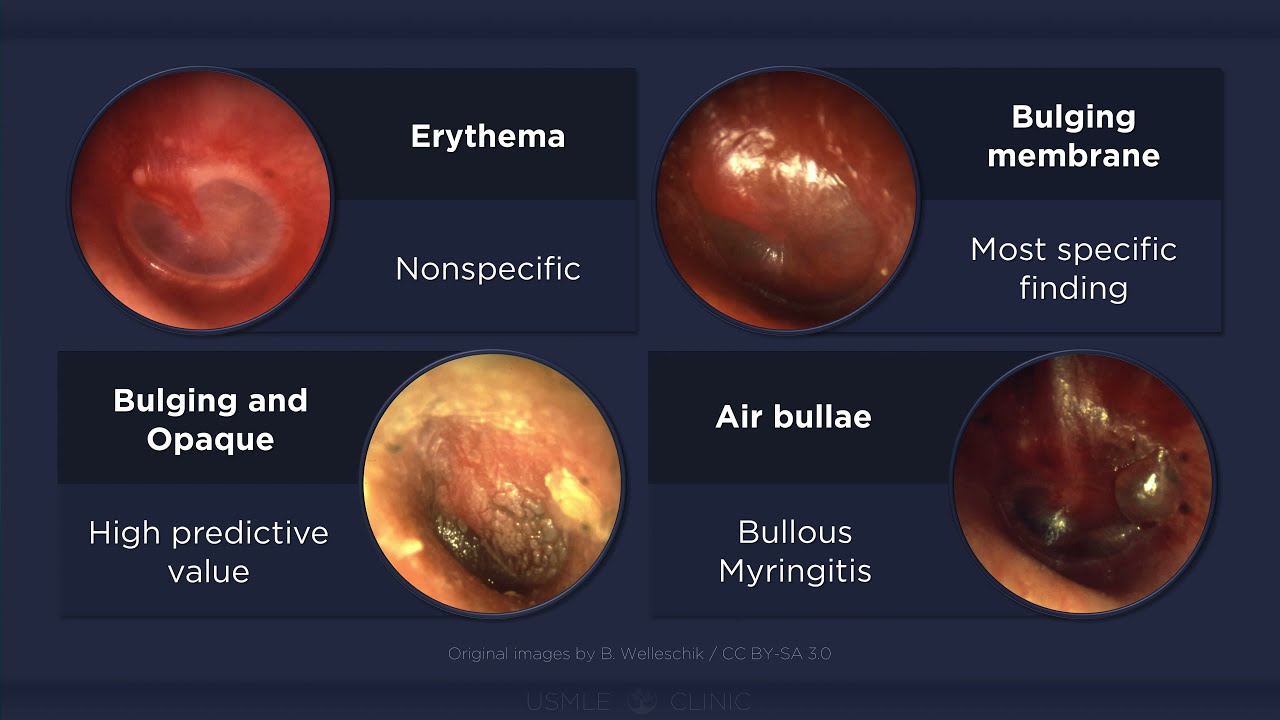
Tympanic Membrane Changes in Otitis Media
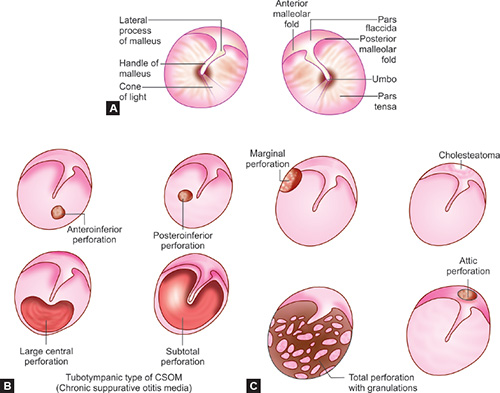
Tympanic Membrane Perforation
Nose
Inspect the nasal passages for:
- Obstruction or congestion
- Discharge or epistaxis
- Deviated septum or structural abnormalities
- Foreign bodies
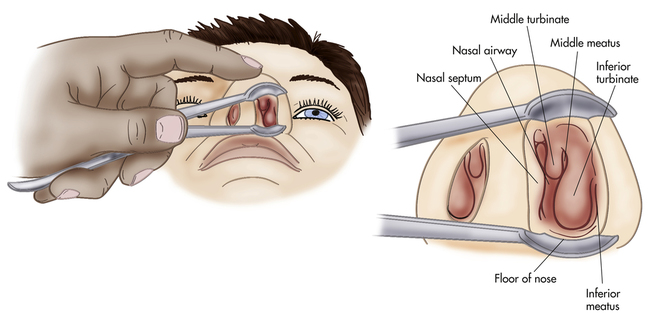
Normal Nasal Examination
Throat
Use a tongue depressor and light to examine:
- Redness, swelling or exudates
- Tonsillitis or pharyngitis
- Ulcers or oral lesions
- Foreign bodies
- Dysphagia
- Cervical lymphadenopathy
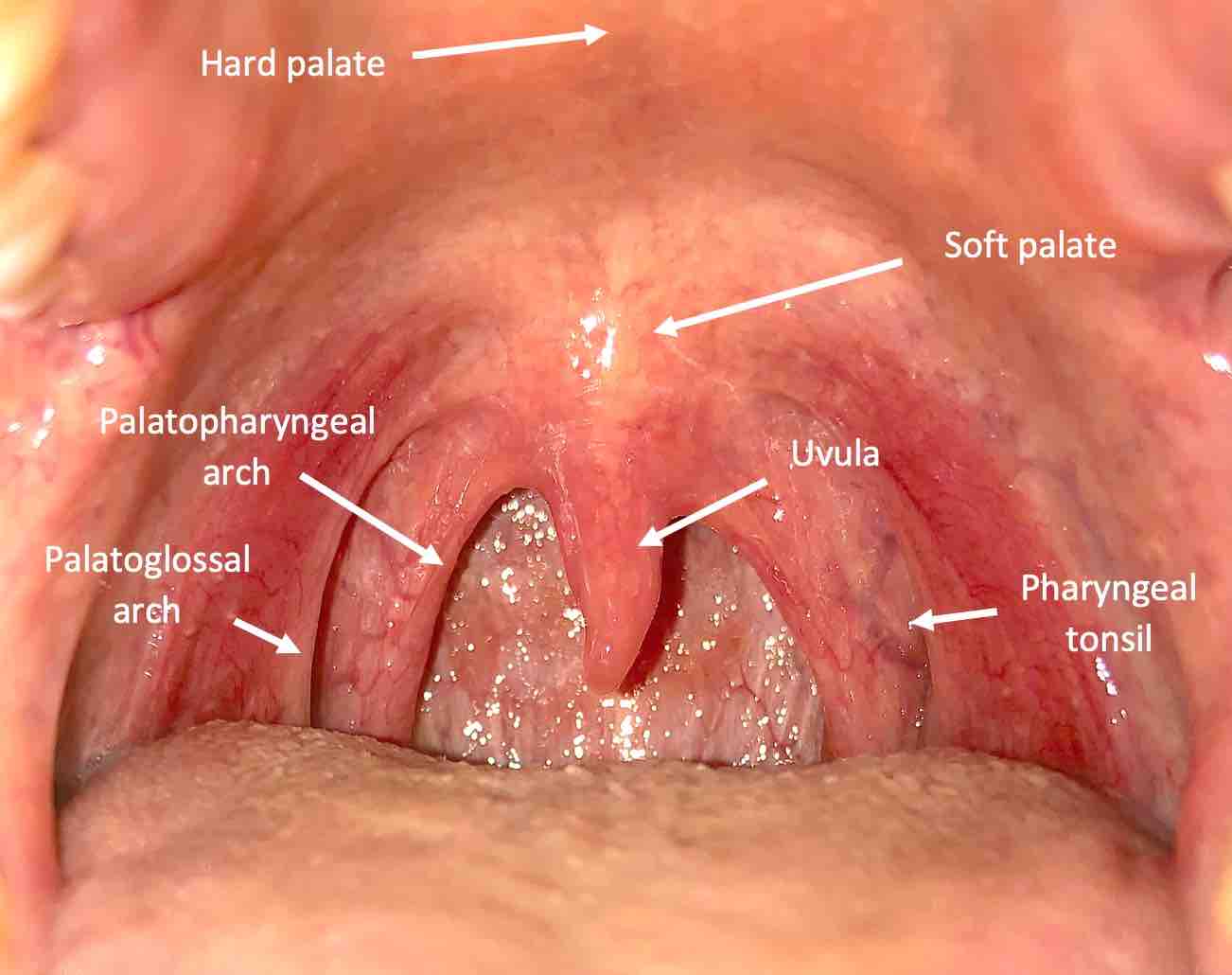
Normal Throat
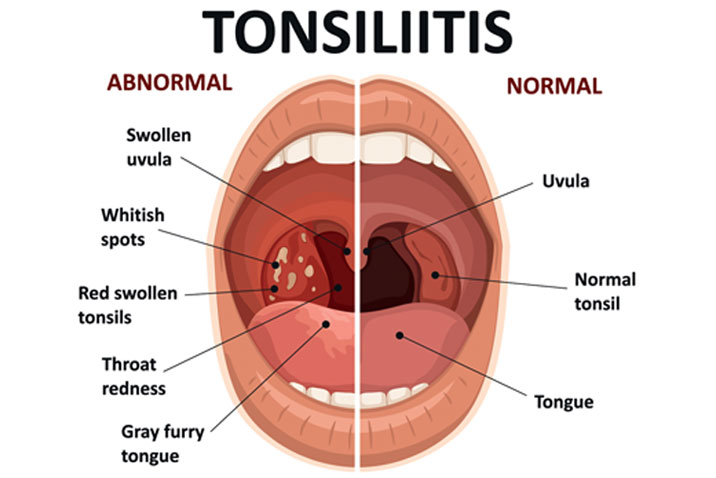
Tonsillitis
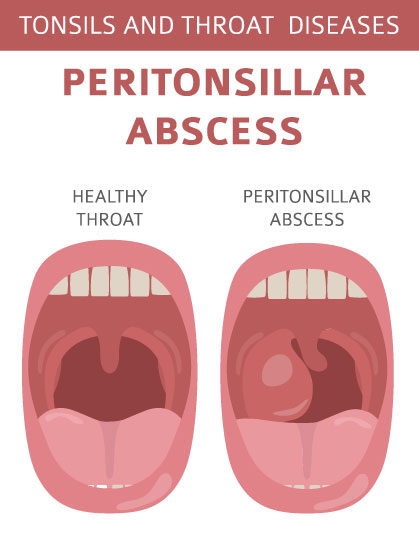
Peritonsillar Abscess (Quinsy)
Diagnostic Evaluation
Further tests may include:
- Pediatric audiometry
- CT or MRI imaging
- Flexible nasopharyngoscopy
- Throat or nasal swab cultures
Pediatric ENT Red Flags
These features should prompt urgent senior review, possible ENT referral, and consideration for admission:
- Stridor, noisy breathing, or any signs of respiratory distress (retractions, tachypnoea, hypoxia).
- Drooling, inability to handle secretions, tripod position, or very painful swallowing.
- Muffled “hot potato” voice, trismus, or severe unilateral throat pain (suggesting quinsy or deep neck infection).
- Rapidly enlarging neck swelling, torticollis, or obvious neck asymmetry.
- Mastoid tenderness, swelling, or protruding pinna suggesting mastoiditis.
- Persistent unilateral foul-smelling or bloody nasal discharge (possible foreign body or mass).
- Sudden onset hearing loss or facial nerve weakness.
- Systemic toxicity: high fever, lethargy, poor feeding, altered mental status, or signs of sepsis.
- Very young infants (<3 months) with fever and any ENT focus.
Quick Pediatric ENT Algorithm for A&E
Use this as a quick mental flow in the Emergency Department:
-
Initial Impression: Sick or Not Sick?
- Check ABCDE immediately.
- If any airway or breathing compromise → call for senior help, anaesthetics/ENT, prepare for airway support.
-
Airway/Breathing Symptoms Present?
- Stridor / respiratory distress: High flow oxygen, nebulised adrenaline if indicated, steroids, keep child calm, early ENT/anaesthetics.
- Drooling / inability to swallow / tripod position: Do not attempt aggressive oral examination, keep child upright, urgent ENT and anaesthetics.
-
If Airway Stable – Identify Main Complaint
- Ear pain / discharge: Consider otitis media/externa, foreign body, TM perforation.
- Sore throat: Tonsillitis, pharyngitis, quinsy, viral URTI.
- Nasal symptoms: Rhinitis, sinusitis, epistaxis, nasal foreign body.
- Hearing or speech delay: Glue ear, conductive hearing loss, sensorineural loss.
-
Look for Red Flags
- If any present → escalate, consider imaging, IV antibiotics, admission.
- If no red flags and child well → manage as outpatient with safety netting.
-
Decide on Disposition
- Admit: Airway/breathing issues, systemic toxicity, severe pain not controlled, concern for mastoiditis, quinsy, deep neck space infection.
- Discharge: Stable child, no red flags, clear diagnosis, caregiver understands red flags and follow-up advice.
Common Pediatric ENT Emergencies
Key emergencies you will often see in A&E and their initial management priorities:
1. Stridor & Acute Upper Airway Obstruction
- Keep child with caregiver, avoid upsetting them.
- High flow oxygen, consider nebulised adrenaline if indicated.
- Give systemic steroids if appropriate (e.g. dexamethasone).
- Urgent ENT/anaesthetic review for potential airway intervention.
- Do not force the child to lie flat or cry unnecessarily.
2. Inhaled or Impacted Foreign Body (Airway)
- Sudden onset cough, wheeze, or unilateral decreased air entry.
- If complete obstruction and child conscious → age-appropriate choking algorithm (back blows, chest/abdominal thrusts).
- If partial obstruction and stable → avoid blind sweeps, urgent ENT/anaesthetics for bronchoscopy.
- Consider imaging but do not delay airway management.
3. Nasal Foreign Body
- Common in toddlers; unilateral foul-smelling or bloody discharge.
- If visible and cooperative child → consider simple removal in ED (parent’s kiss technique, suction, hook) if trained and safe.
- Avoid pushing object further back.
- ENT referral if not easily removed, if button battery, or if penetrating object.
4. Epistaxis
- Sit child up, head slightly forward, pinch soft part of nose continuously for 10–15 minutes.
- Reassure child and caregiver, avoid swallowing blood.
- Consider topical vasoconstrictor and local pressure if persistent.
- ENT referral for recurrent, severe, or posterior bleeds.
5. Tonsillitis & Peritonsillar Abscess (Quinsy)
- Severe sore throat, trismus, muffled “hot potato” voice, unilateral swelling, uvula deviation.
- ABC assessment – ensure no airway compromise.
- IV fluids, analgesia, antibiotics if indicated.
- ENT referral for drainage of quinsy and admission if unwell.
6. Mastoiditis
- Post-auricular swelling, erythema, tenderness, protruding pinna, often following otitis media.
- Systemically unwell child, fever, irritability.
- Urgent ENT referral, IV antibiotics, and imaging if required.
7. Deep Neck Space Infection
- Neck swelling, torticollis, severe pain, fever, drooling, trismus.
- Airway evaluation is the first priority.
- IV antibiotics, imaging (CT neck with contrast if safe), urgent ENT and anaesthetics.
Always document red flags, safety net advice, and review arrangements clearly in the notes.